Reduction in liver iron concentration (LIC)
FIRST Study: A controlled non-inferiority study of patients with sickle cell disease and other transfusion-dependent anemias evaluated the change in liver iron concentration (LIC) after 12 months of treatment with Ferriprox vs. deferoxamine.1,2†
There were no significant treatment group differences at baseline or after 12 months (96.01% CI) and the non-inferiority criterion was met.1
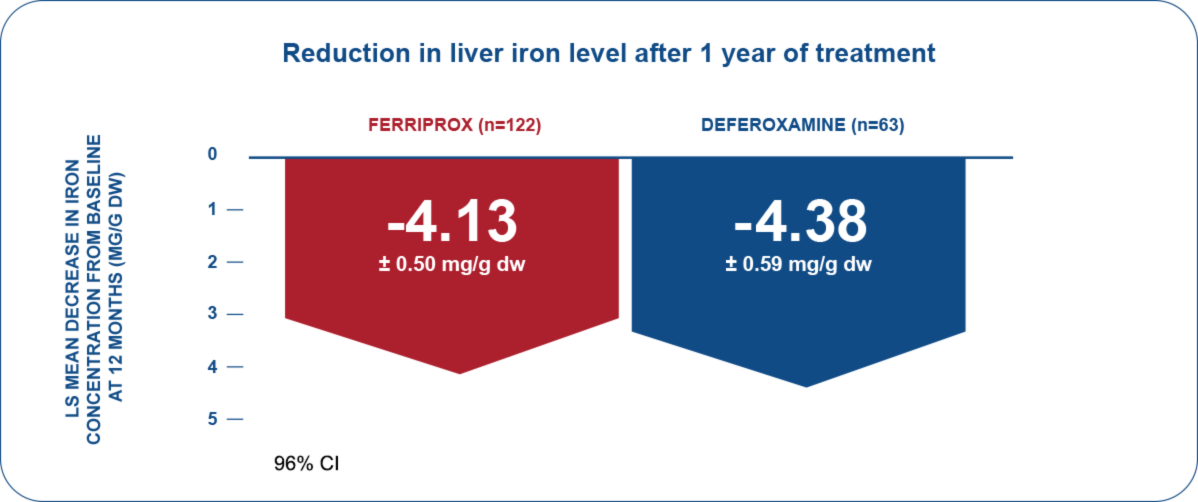
† The non-inferiority criterion was established as the upper limit of the 96.01% confidence interval for the difference between treatments being ≤2 mg/g dry weight (dw).
CI = Confidence Interval
Effective liver iron reduction
FIRST-EXT Study: Patients who completed the non-inferiority study and enrolled in a 2-year extension study either continued to receive Ferriprox (n=89 patients), or were switched to Ferriprox from deferoxamine (n=45 patients) .1,2
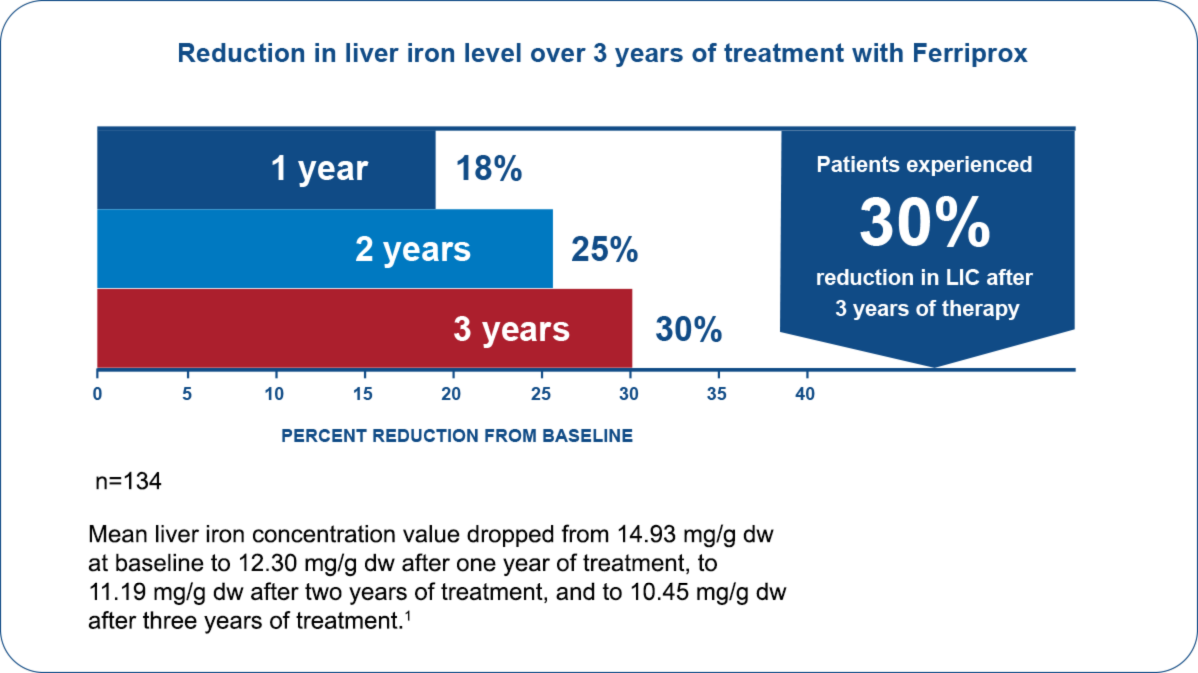
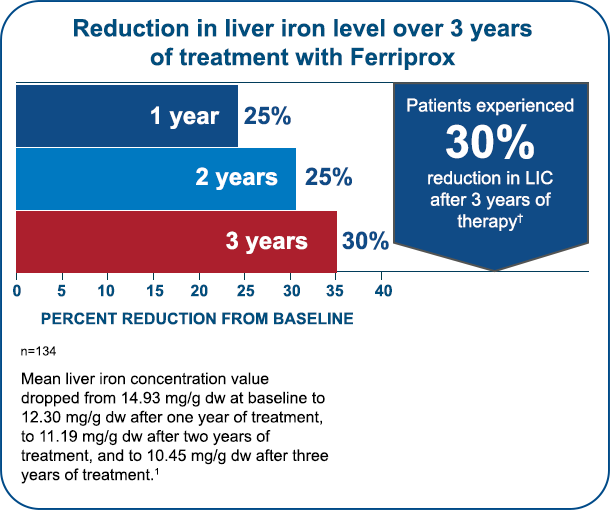
Continuous liver iron reduction
IMPORTANT SAFETY INFORMATION
Indication
Ferriprox® (deferiprone) is an iron chelator indicated for the treatment of transfusional iron overload in patients with:
- thalassemia syndromes
- sickle cell disease or other anemias
Ferriprox Tablets are indicated in adult and pediatric patients ≥8 years of age; Ferriprox Oral Solution is indicated in patients ≥3 years of age.
Limitations of Use:
Safety and effectiveness have not been established for the treatment of transfusional iron overload in patients with myelodysplastic syndrome or in patients with Diamond Blackfan anemia.
WARNING: AGRANULOCYTOSIS AND NEUTROPENIA
- Ferriprox can cause agranulocytosis that can lead to serious infections and death. Neutropenia may precede the development of agranulocytosis.
- Measure the absolute neutrophil count (ANC) before starting Ferriprox and monitor regularly while on therapy.
- Interrupt Ferriprox therapy if neutropenia develops.
- Interrupt Ferriprox if infection develops, and monitor the ANC more frequently.
- Advise patients taking Ferriprox to report immediately any symptoms indicative of infection.
Indication
Ferriprox® (deferiprone) is an iron chelator indicated for the treatment of transfusional iron overload in patients with:1
- thalassemia syndromes
- sickle cell disease or other anemias
Ferriprox Tablets are indicated in adult and pediatric patients ≥8 years of age; Ferriprox Oral Solution is indicated in patients ≥3 years of age.
Limitations of Use:
Safety and effectiveness have not been established for the treatment of transfusional iron overload in patients with myelodysplastic syndrome or in patients with Diamond Blackfan anemia.
Important Safety Information
Ferriprox is contraindicated in patients with known hypersensitivity to deferiprone or to any of the excipients in the formulations.
In pooled clinical trials, 7.5% of 642 patients with thalassemia syndromes treated with Ferriprox developed increased ALT values. Four (0.62%) Ferriprox-treated subjects discontinued the drug due to increased serum ALT levels and 1 (0.16%) due to an increase in both ALT and AST. In pooled clinical trials, 7.7% of 196 patients with sickle cell disease or other anemias treated with Ferriprox developed increased ALT values. Monitor serum ALT values monthly during therapy with Ferriprox and consider interruption of therapy if there is a persistent increase in the serum transaminase levels. Decreased plasma zinc concentrations have been observed on deferiprone therapy. Monitor plasma zinc annually, and supplement in the event of a deficiency.
Ferriprox can cause fetal harm. Advise females of reproductive potential to use an effective method of contraception during treatment with Ferriprox and for at least six months after the last dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with Ferriprox and for at least three months after the last dose. Advise females not to breastfeed during treatment with Ferriprox and for at least 2 weeks after the last dose.
Avoid co-administration of Ferriprox with other drugs known to be associated with neutropenia or agranulocytosis; however, if this is unavoidable, closely monitor the absolute neutrophil count. Avoid co-administration with UGT1A6 inhibitors. Allow at least a 4-hour interval between administration of Ferriprox and drugs or supplements containing polyvalent cations (e.g., iron, aluminum, or zinc).
The most common adverse reactions in patients with thalassemia (incidence ≥6%) are nausea, vomiting, abdominal pain, arthralgia, ALT increased and neutropenia. The most common adverse reactions in patients with sickle cell disease or other anemias (incidence ≥6%) are pyrexia, abdominal pain, bone pain, headache, vomiting, pain in extremity, sickle cell anemia with crisis, back pain, ALT increased, AST increased, arthralgia, oropharyngeal pain, nasopharyngitis, neutrophil count decreased, cough and nausea.
Inform patients that their urine might show a reddish/brown discoloration due to the excretion of the iron-deferiprone complex. This is a very common sign of the desired effect, and it is not harmful.
Advise patients to avoid alcohol while taking Ferriprox tablets (twice-a-day). Consumption of alcohol while taking Ferriprox tablets (twice-a-day) may result in more rapid release of deferiprone.
Please see Full Prescribing Information, including boxed WARNING, and Medication Guide.
IMPORTANT SAFETY INFORMATION
Indication
Ferriprox® (deferiprone) is an iron chelator indicated for the treatment of transfusional iron overload in patients with:
- thalassemia syndromes
- sickle cell disease or other anemias
Ferriprox Tablets are indicated in adult and pediatric patients ≥8 years of age; Ferriprox Oral Solution is indicated in patients ≥3 years of age.
Limitations of Use:
Safety and effectiveness have not been established for the treatment of transfusional iron overload in patients with myelodysplastic syndrome or in patients with Diamond Blackfan anemia.
WARNING: AGRANULOCYTOSIS AND NEUTROPENIA
- Ferriprox can cause agranulocytosis that can lead to serious infections and death. Neutropenia may precede the development of agranulocytosis.
- Measure the absolute neutrophil count (ANC) before starting Ferriprox and monitor regularly while on therapy.
- Interrupt Ferriprox therapy if neutropenia develops.
- Interrupt Ferriprox if infection develops, and monitor the ANC more frequently.
- Advise patients taking Ferriprox to report immediately any symptoms indicative of infection.
Indication
Ferriprox® (deferiprone) is an iron chelator indicated for the treatment of transfusional iron overload in patients with:1
- thalassemia syndromes
- sickle cell disease or other anemias
Ferriprox Tablets are indicated in adult and pediatric patients ≥8 years of age; Ferriprox Oral Solution is indicated in patients ≥3 years of age.
Limitations of Use:
Safety and effectiveness have not been established for the treatment of transfusional iron overload in patients with myelodysplastic syndrome or in patients with Diamond Blackfan anemia.
Important Safety Information
Ferriprox is contraindicated in patients with known hypersensitivity to deferiprone or to any of the excipients in the formulations.
In pooled clinical trials, 7.5% of 642 patients with thalassemia syndromes treated with Ferriprox developed increased ALT values. Four (0.62%) Ferriprox-treated subjects discontinued the drug due to increased serum ALT levels and 1 (0.16%) due to an increase in both ALT and AST. In pooled clinical trials, 7.7% of 196 patients with sickle cell disease or other anemias treated with Ferriprox developed increased ALT values. Monitor serum ALT values monthly during therapy with Ferriprox and consider interruption of therapy if there is a persistent increase in the serum transaminase levels. Decreased plasma zinc concentrations have been observed on deferiprone therapy. Monitor plasma zinc annually, and supplement in the event of a deficiency.
Ferriprox can cause fetal harm. Advise females of reproductive potential to use an effective method of contraception during treatment with Ferriprox and for at least six months after the last dose. Advise males with female partners of reproductive potential to use effective contraception during treatment with Ferriprox and for at least three months after the last dose. Advise females not to breastfeed during treatment with Ferriprox and for at least 2 weeks after the last dose.
Avoid co-administration of Ferriprox with other drugs known to be associated with neutropenia or agranulocytosis; however, if this is unavoidable, closely monitor the absolute neutrophil count. Avoid co-administration with UGT1A6 inhibitors. Allow at least a 4-hour interval between administration of Ferriprox and drugs or supplements containing polyvalent cations (e.g., iron, aluminum, or zinc).
The most common adverse reactions in patients with thalassemia (incidence ≥6%) are nausea, vomiting, abdominal pain, arthralgia, ALT increased and neutropenia. The most common adverse reactions in patients with sickle cell disease or other anemias (incidence ≥6%) are pyrexia, abdominal pain, bone pain, headache, vomiting, pain in extremity, sickle cell anemia with crisis, back pain, ALT increased, AST increased, arthralgia, oropharyngeal pain, nasopharyngitis, neutrophil count decreased, cough and nausea.
Inform patients that their urine might show a reddish/brown discoloration due to the excretion of the iron-deferiprone complex. This is a very common sign of the desired effect, and it is not harmful.
Advise patients to avoid alcohol while taking Ferriprox tablets (twice-a-day). Consumption of alcohol while taking Ferriprox tablets (twice-a-day) may result in more rapid release of deferiprone.
Please see Full Prescribing Information, including boxed WARNING, and Medication Guide.
References: 1. Ferriprox® (deferiprone) Prescribing Information. Chiesi, November 2021. 2. Kwiatkowski J et al. Deferiprone vs. deferoxamine for transfusional iron overload in SCD and other anemias: A randomized, open-label, noninferiority study. Blood Advances 2022. Epub ahead of print doi: 10.1182/bloodadvances.2021004938.